Some while ago, I published a video and article about some experiments I did to test for radial nerve sensitivity in the upper cinch area. During my internet forays, I stumbled upon a video by a certain well-known rigger seemingly spreading the very misinformation of which he complains! Maybe one of us is misunderstanding the other? I do hope so and that he is not as seriously misinformed as he appears. However, the important thing is we get a better understanding of the subject rather than seek to score points.
As he says, “Look for real medical information.“. He asked a doctor for his opinion. So, I asked a surgeon, whose speciality is the upper limbs, and has also been doing suspensions for some years. I guess that’s as real as it gets.
The idea of the experiment was try to simulate the sort of pressure that might be caused by rope in the armpit area. The most obvious example of this would be the upper cinches in a typical gote but, of course, there are other situations where a rope could cause pressure in this area and even a gote might involve different arm positions, e..g. dropped arms, high hands or even reverse.
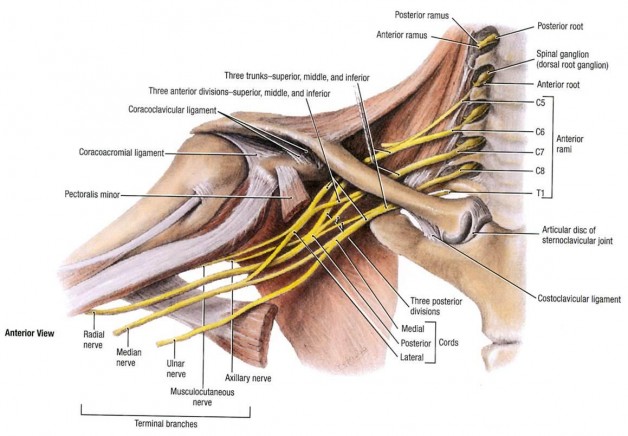
Changing arm position might give better results for specific ties but that’s an area for further experimentation. Speaking for myself, and a couple of others, it produced sensations shooting to thumb and forefinger at some stage, depending of the bulk, which indicate pressure on the radial. Pressure on the radial nerve usually causes symptoms in the back of the hand, near the thumb, and in the index and middle fingers, whereas median causes symptoms in the thumb, index, and middle fingers, and medial half the ring finger. Yes, I know that sounds pretty much the same but when you see it expressed schematically, the difference becomes clear:

My critic seems to deny a risk in the cinch area. This surprises me as not only does the diagram (below), which he references, specifically illustrate this but it seems well-known as a danger area. Whilst it was by no means the first I’d heard of it, I recall Kazami Ranki discussing it at some length during his 5-day workshop.
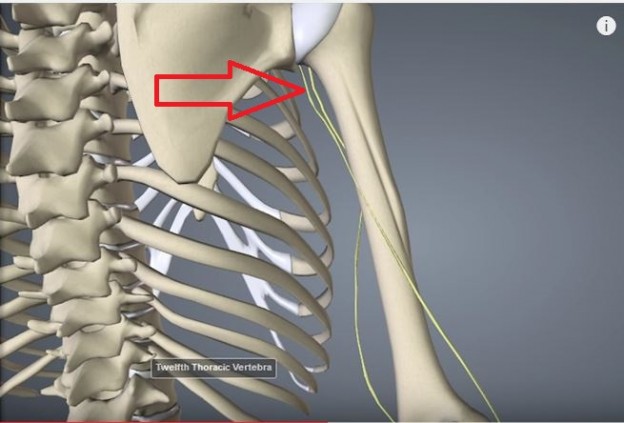
You can see the proximity of the radial and median nerves in the upper cinch area, indicated by the arrow. As you’ll learn, being close to the bone means it can be trapped against it. I speculate that this is what my test does.
Just to make sure, I raised this with my surgeon friend, submitting both videos. This is what he said about the medical aspects:
“The brachial plexus is made from five roots (C5to T1), which branches into three cords (medial, lateral and posterior), cords which branches into 5 nerves, the most important for the upper limb being the radial, median and ulnar nerves. At the armpit level, i.e. the zone where the upper cinches are located the cords are already divided into nerves. The median and ulnar nerves stay medially to the humeral bone and the radial goes behind this bone.
At the level of the upper cinches, the three nerves are still medial to the humeral bone, and then may be crushed between something and the bone. In my everyday practice, I see anaesthesiologists blocking the three nerves by injecting local anaesthetics at the level. The radial nerve is the deepest which means closest to the bone. The other nerves are more superficial, and surrounded by soft tissues, which explains maybe why the radial nerve is more sensitive than the others. I don’t know if this test is precise for radial nerve sensitivity, but I do know that it is obvious that this region is a sensitive region where three major nerves are located and that the radial nerve is more sensitive than the others, as attested by the “Saturday night palsy”.”
http://www.assh.org/handcare/hand-arm-injuries/Brachial-Plexus-Injury
http://www.ncemi.org/cse/cse0919.htm
http://www.nysora.com/techniques/nerve-stimulator-and-surface-based-ra-techniques/upper-extremitya/3262-cutaneous-nerve-blocks-of-the-upper-extremity.html
He went on to say:
“Yes, maybe making the test in a gote position would improve its efficiency, but I can’t advice to make or not upper cinches [based on the] results of the test. I believe it’s a danger zone, and it’s best to avoid upper cinches. The question for me is rather: do we really need upper cinches?”
Good question. Are upper cinches essential? No, of course not. There are numerous variants on the gote, the classic Akechi derived version is the one most know. Whilst not true to the style, it is quite possible to use one without the upper cinches. Old-stle gotes are often without upper cinches, this function often being performed by a central rope at the front. Good examples are Marai Masato’s, Naka Akira’s versions.

So, to be clear, he says “I don’t know if this test is precise for radial nerve sensitivity”. Nor do I but we are not talking about expensive hospital machines here 🙂 However, I would emphasise, it is extremely useful if you can produce sensations that will allow you to recognise warning signs. Know your enemy! That way, you can act as soon as you feel the slightest twinge and not when it’s too late.
As a predictive test, I would go no further than to say that it could help you identify sensitivities and how much is too much in terms of bulk. There is no doubt that palpation is about the only way we can determine nerve positions and sensitivity without diagnostic equipment. The test attempts to use this principal by mimicking the real life situation more accurately by use of fingers, rope or other objects. As my surgeon friend implies, the test could be tried in different positions to improve results. We know that very little we do can ever be expressed with precise rules since everyone is slightly different. How would I use this test? Well, if sensations were produced by very little bulk, I’d be especially cautious about this area, in the same way that if palpation revealed undue sensitivity. I would be very interested to receive feedback on your experiences.