A recent discussion on my Fetlife kinbaku group threw up an interesting misnomer concerning the potential nerve vulnerability on the inner side of the arm. It’s quite possible we were talking at cross purposes but since “The TK” (actually a whole family of ties) is getting some undeservedly bad press, I think it’s worth clarifying where nerves are most vulnerable in the upper arm. In my opinion, inner side of the upper arm is one of the two major sites of box-tie suspension injuries (marked A below). In this area, the radial, median and ulnar pass from the spine in a bundle, called the brachial plexus, under the armpit to branch out down the arm. I devised a way to test for radial sensitivity which can be combined with palpating to locate the nerve. I wrote about it here and posted a video.
The other main cause of radial compression is pressure from the lower wraps due to bad placement or movement. You can see the radial run down the inside of the upper arm and spiral around at around the top of the lower third (in the region of B below). You can read more about the vulnerability there from the lower wrap in this article. In short:
- Watch out for bulk, e.g. knots, twists, bunched up clothing, in the upper cinch under the arm
- Never cinch between the back and front of a wrap as this forms a ligature around the arm
- Keep cinch ropes under minimal tension
- Allow upper wrap to lock under shoulder blades and base of deltoid
- Keep lower wrap up and away from the radial
For general upper body information, see my Nerve Damage Study. I strongly recommend study of BioDigital Human which allows exploration of human anatomy via annotated 3D images.
BEWARE!
No two people are the same and you will not be identical to the diagram below. It is essential to be sure where your nerves run and make sure the rigger takes this into account. If he doesn’t or the tie fails in its functionality, don’t blame the tie. This is like blaming a car manufacturer for accidents resulting from bad driving or inadequate maintenance. However, even a perfect driver in a perfect car can still have an accident. Same rules apply to suspension bondage.
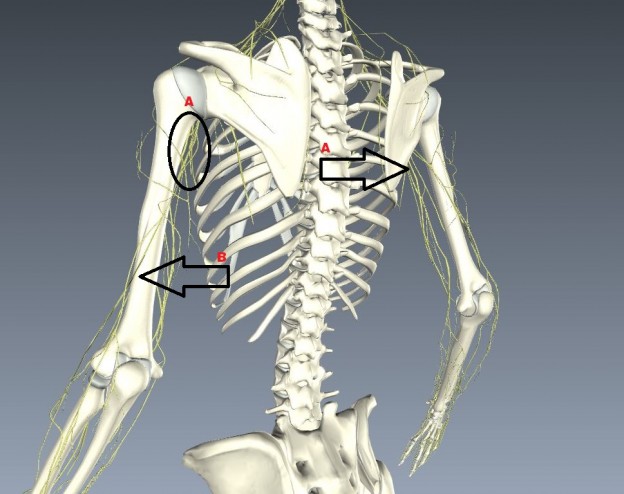
Rear view from BioDigitalHuman.com
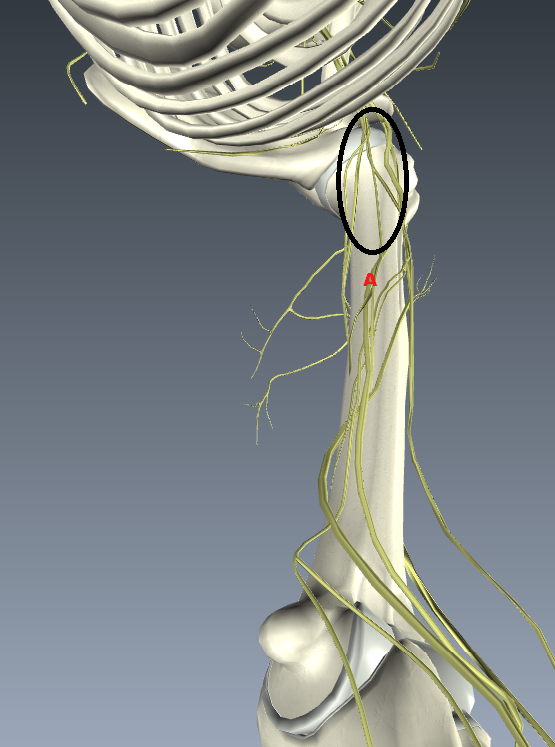
Beneath view from BioDigitalHuman.com
Causes of injury
- The radial nerve may be damaged by trauma or entrapped, especially between the heads of muscles.
- In the axilla:
- With features of weak triceps, wrist drop and possibly also median and ulnar nerve involvement. The most common cause is compression.
- The radial nerve may be damaged in the axilla by fracture or dislocation of the head of the humerus.
- Saturday night syndrome (so named because it can be acquired by sleeping with the arm over the back of a chair whilst in a drunken stupor, so compressing the plexus):
- Is due to compression of the lower part of the brachial plexus. As this is really a brachial plexus injury, the median and ulnar nerves may also be involved.
- It may also be compressed by the use of shoulder crutches.
- Nerve function usually fully recovers within a few weeks.
- In the upper arm (triceps and brachioradialis are often spared):
- May be due to a compression lesion but fracture is the usual cause. Injections given in the arm of small babies can damage the radial nerve.
- As the nerve often passes down in the spiral groove of the humerus, it may be injured with a fracture of the shaft of the humerus.
- At the elbow:
- The radial nerve may be entrapped at the elbow at a number of sites but the most common is the proximal border of the tendon of supinator called the arcade of Frohse.
- Check for tenderness over the radial tunnel. There may be pain when the fingers are extended against resistance.
- Supination from a pronated position along with flexion of the wrist may reproduce the symptoms.
- Lesions at the wrist:
- Cause finger drop with a normal wrist and intact sensation.
- Causes include fracture of the radius, elbow deformity, soft-tissue masses and compression by the extensor carpi radialis brevis.
- Lesions of the superficial nerves (cause pain and sensory loss but no motor loss):
- At the elbow, ruptured synovial effusion is the most common cause. In the forearm there may be an aberrant course through the muscles.
- At the wrist, causes include compression from plaster casts, wristbands or handcuffs, especially the type that get tighter with struggling. Other causes are surgery, injections and nerve tumours.
Symptoms
Based on the location of the nerve damage, brachial plexus injuries can affect part of or the entire arm. For example, musculocutaneous nerve damage weakens elbowflexors, median nerve damage causes proximal forearm pain, and paralysis of the ulnar nerve causes weak grip and finger numbness.[7] In some cases, these injuries can cause total and irreversible paralysis. In less severe cases, these injuries limit use of these limbs and cause pain.[8]
The cardinal signs of brachial plexus injury then, are weakness in the arm, diminished reflexes, and corresponding sensory deficits.
See Brachial Plexus Assessment and Common Injuries for full text of the extracts below.
Sensory nerves:
Pinch the nail base, pull the finger outwards and ask about feeling anything. A burning feeling indicates continuity in the following nerves; absence does not necessarily mean nerve is divided but may be due to neurapraxia instead.
- Thumb – tests the median nerve supplied by C6.
- Middle finger – tests the median nerve supplied by C7.
- Little finger – tests the ulnar nerve suppled by C8.
Motor nerves:
Examination can be made difficult by anomalous nerve distribution, including C4 contributing to the brachial plexus and also because many muscles are supplied by more than one motor neuron. Assessment of loss of motor function at the cervical root:
- C5: shoulder movement in all directions, flexion of elbow (to some degree).
- C6: flexion of elbow, rotation of forearm, flexion of wrist (to some degree).
- C7: mainly a sensory trunk. (Produces generalised loss of movement in the arm, without total paralysis in any given muscle group. Always supplies the latissimus dorsi.)
- C8: extension and flexion of fingers, flexion of wrist, hand movement.
- T1: intrinsic muscles of the hand, eg adduction or abduction of fingers.
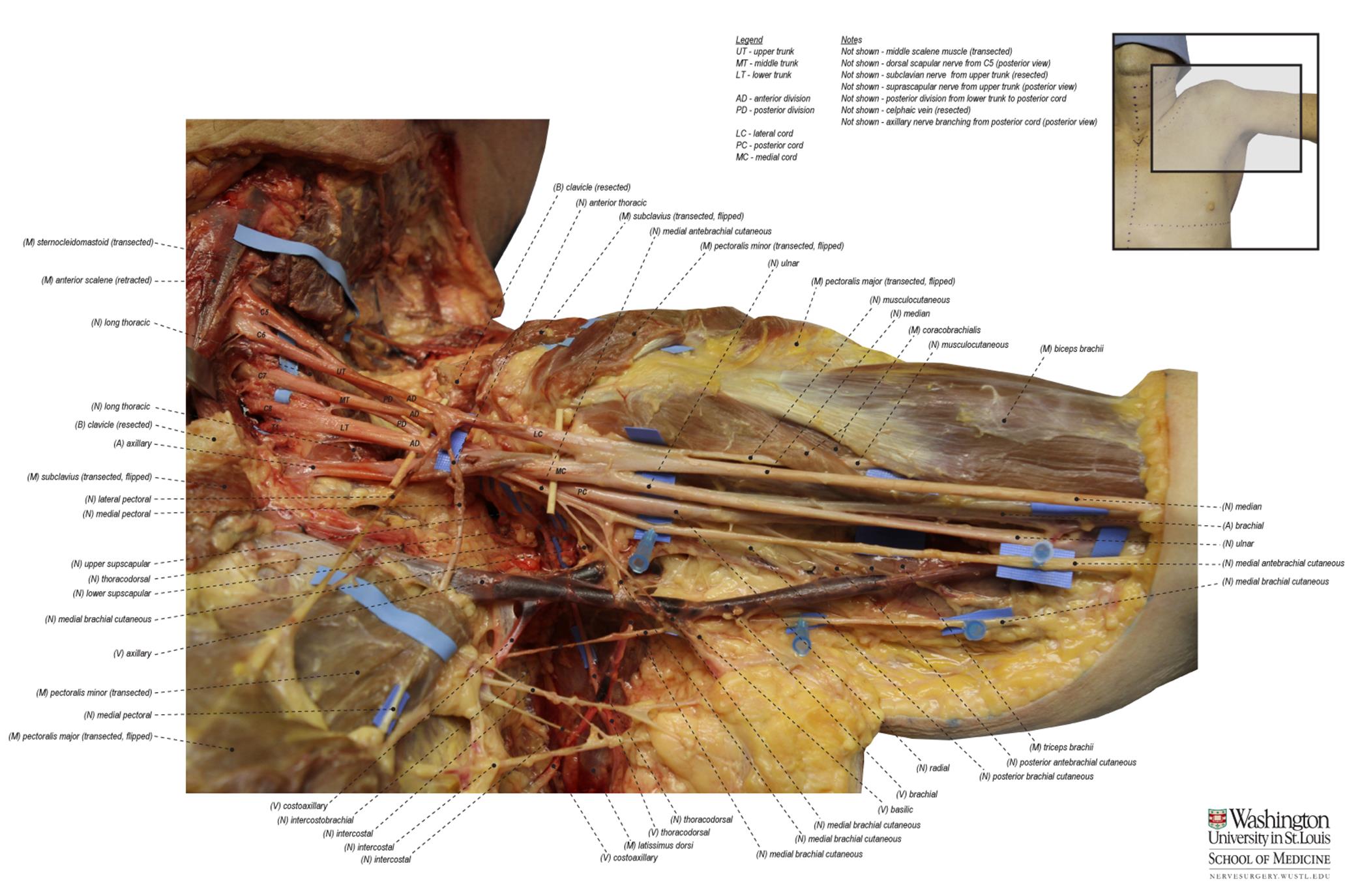
Dissection of brachial plexus. Click to enlarge